Growing up in an African community, I always heard stories of women struggling with infertility because they had fibroids. These women complained of painful periods, heavy periods, bloating, and miscarriages. This article aims to shed light on fibroids and how these benign uterine tumors affect fertility.

What are fibroids?
Fibroids occur when the uterus’s muscular tissue develops a benign (noncancerous) tumor. These benign uterine tumors are also known as myomas and leiomyomas.
Fibroids may be problematic because they alter the size and shape of the uterus and, occasionally, the cervix. Most women have multiple fibroids, but some can have just one. The position, size, and number of fibroids determine whether they are symptomatic or need to be treated.
Although they occasionally occur in the cervix, fibroids are typically located in or near the uterus’s body.
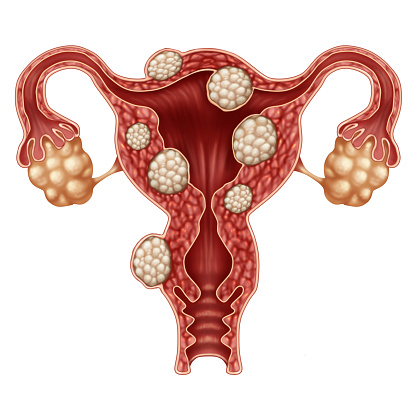
Types of fibroids
Subserosal: These fibroids are on the uterus’s exterior wall (55%)
Intramural: These fibroids are in the muscular layers of the uterine wall( 40%)
Submucosal: These fibroids protrude into the uterine cavity (5%)
Fibroids can also be attached to neighboring ligaments or organs, such as the bladder and colon, or connected to the uterus via a stalk (pedunculated). Seldom are fibroids discovered outside of the pelvic cavity.
What is the prevalence of fibroids?
20% of women of reproductive age have fibroids, but black women (between 50% and 80%) have more. Uterine fibroids may have a variety of genetic, hormonal, and environmental causes. However, the exact causes are unknown.
Does having fibroids affect fertility?
Fibroids are present in 5% to 10% of infertile women. Whether fibroids have an impact on fertility depends on their size and location. Examples include massive (>6 cm in diameter) uterine wall fibroids or submucosal fibroids inside the uterine cavity.
Most women with fibroids won’t have trouble getting pregnant. However, women with fibroids should be evaluated for other fertility issues before commencing fibroid treatment. A fertility expert will help determine the fibroids are the cause of infertility.
How do fibroids result in infertility?
Uterine fibroids can decrease fertility in several ways, including:
- Changes in the shape of the cervix might reduce the amount of sperm that can enter
- The migration of the sperm or embryo can be hampered by changes in the uterus’s shape.
- Fibroids may obstruct fallopian tubes
- Fibroid may affect how thick the uterine cavity lining is
- Fibroids might alter the uterine cavity’s blood flow hindering the embryo’s ability to attach to the uterine wall
Can getting rid of fibroids make you more fertile?
Some patients may experience improved fertility after eliminating fibroids with uterus-preserving procedures. However, the primary goal of fibroid removal is to relieve symptoms like excessive bleeding and bloating.
Can someone with fibroids still become pregnant?
A lot of people who have fibroids can become pregnant. However, discussing your objectives and top priorities with your doctor is advisable to increase your chances of having a safe pregnancy. In addition, a gynecologic surgeon can talk to you about treatment choices to help maintain your fertility if fibroids negatively affect your quality of life.
What happens to fibroids once a woman is pregnant?
About 2% to 12% of pregnant women have fibroids. However, not all fibroids enlarge or create issues. Most fibroids grow during the first trimester of pregnancy.
What risks do pregnant women with fibroids have?
- Fibroids may raise the risk of preterm birth or miscarriage
- Fibroids may get bigger than their blood supply, resulting in severe pain.
- Fibroids can also alter the location of the fetus within the uterus.
Your physician will help determine how the fibroids are managed depending on your situation. Pregnancy rarely necessitates or requires surgery.
After removing a fibroid, a woman should talk to the obstetrician who will deliver the baby if she becomes pregnant. It could be advised to have a cesarean section.
Which fibroid therapies improve fertility?
Myomectomy is the gold standard treatment for younger patients with fibroids who want to keep their fertility. Unlike a hysterectomy, a myomectomy spares your uterus, so you can still get pregnant following the treatment. A single, big incision can perform a myomectomy, but physicians prefer minimally invasive methods like robotic surgery and laparoscopic surgery.
You may be a candidate for a myomectomy, depending on several criteria. These criteria are:
- The location of your uterine fibroid(s)
- How big your fibroid is (s)
- how many fibroids you have
- Your general well-being
How are fibroids managed or removed while pregnant?
Doctors cannot remove fibroids during pregnancy, but they can help you manage your symptoms.
Is it possible to have a “normal” or “natural” delivery if you have fibroids?
Most people with fibroids can give birth naturally (delivery through the vagina). Fibroids do, however, raise the possibility of a C-section. Contrary to pregnant women without fibroids, individuals with fibroids are six times more likely to require a C-section.
Do fibroids naturally disappear after giving birth?
Fibroids frequently increase during pregnancy and frequently shrink after birth. Nonetheless, some people might still have fibroids symptoms like heavy periods and bloating. Some treatments may help you if you continue to have these symptoms.
In conclusion
Fibroids can have a negative impact on your fertility in different ways. They can influence conception, the ability of an embryo to implant, the continuation of a pregnancy, and the development and position of the fetus.
Each patient’s course of treatment is chosen individually. It is based on fibroids’ symptoms, and these treatments could increase fertility. Your physician’s suggestions and the severity of your symptoms will determine how and whether you should treat your fibroids.
Did you find this article helpful? Leave a comment in the section below.